Principles & Practice of Health Evangelism
Chapter 5
Where Are the Baptisms?
Textbook pages 24-33
Over the years of conducting health evangelism programs I have repeatedly been asked, “Where are the baptisms?” This is a fair question. Pastors and church administrators are interested in numbers that indicate church growth. A person is counted as an authentic member of the church once baptism has taken place.
Conventional health education programs are not designed to be evangelistic. Many health education programs are conducted by church members in an entirely secular manner in a secular setting. It is not to be expected that these programs would be evangelistic or result in baptisms. These more secular programs are rightly accused of creating “healthy sinners.”
Other health education programs have been integrated in some way with traditional evangelistic efforts. In some cases a Five-day Plan to Stop Smoking was held just before an evangelistic crusade in the hopes that the reformed smokers would stay for the doctrinal presentations once they stopped smoking ("Bridging Program"). This never worked very well.
At other times a health segment was included in an evangelistic crusade. A “health nugget” would come before the real meat of the program. This format sometimes increased the crowds, and reformed health habits, but there was only a marginal increase in baptisms.
Over time, most evangelists, not seeing any particular benefit from health education, abandoned the combination of the health message with evangelistic efforts. With the gradual secularization of the church membership at many levels, the whole health message of the church has been abandoned by many church members, and even some pastors, and church administrators.
The problem is not with health evangelism as much as it is with traditional evangelism. What worked well 100 years ago, is no longer effective in drawing crowds into the church. In developed countries where traditional evangelistic crusades have been shown to be less effective now compared with the past, new strategies need to be considered. I believe it is time to take a fresh look at health evangelism.
- What is the relationship between health evangelism and baptisms?
- Should you expect baptisms from health evangelism programs?
Conventional health education programs are not designed to be evangelistic. Many health education programs are conducted by church members in an entirely secular manner in a secular setting. It is not to be expected that these programs would be evangelistic or result in baptisms. These more secular programs are rightly accused of creating “healthy sinners.”
Other health education programs have been integrated in some way with traditional evangelistic efforts. In some cases a Five-day Plan to Stop Smoking was held just before an evangelistic crusade in the hopes that the reformed smokers would stay for the doctrinal presentations once they stopped smoking ("Bridging Program"). This never worked very well.
At other times a health segment was included in an evangelistic crusade. A “health nugget” would come before the real meat of the program. This format sometimes increased the crowds, and reformed health habits, but there was only a marginal increase in baptisms.
Over time, most evangelists, not seeing any particular benefit from health education, abandoned the combination of the health message with evangelistic efforts. With the gradual secularization of the church membership at many levels, the whole health message of the church has been abandoned by many church members, and even some pastors, and church administrators.
The problem is not with health evangelism as much as it is with traditional evangelism. What worked well 100 years ago, is no longer effective in drawing crowds into the church. In developed countries where traditional evangelistic crusades have been shown to be less effective now compared with the past, new strategies need to be considered. I believe it is time to take a fresh look at health evangelism.
Friendship Evangelism
Health evangelism programs, rightly conducted, will lead to baptisms and will elevate the reputation of a church in the community. Health evangelism programs, organized along the lines suggested in this book will make many friends in the community and go a long way toward preparing people for baptism and full church membership.
A survey of recent converts to the church in North America identified various reasons a person joined a church. These are the data:
A survey of recent converts to the church in North America identified various reasons a person joined a church. These are the data:
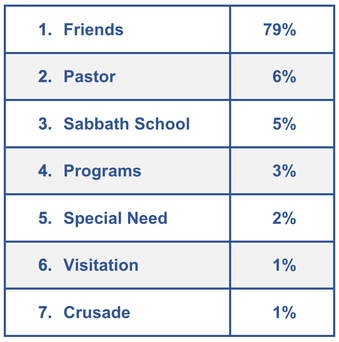
The most important influence in a person joining a church is the presence of personal friends in the congregation. Health evangelism programs, when conducted correctly, create friendships between the public and church members. Health evangelism programs should be designed to create an active, meaningful, interface between church members and individuals in the community.
Soul-saving friendships can be built in small groups that meet each session of a health evangelism program. Lasting friendships with men and women from the community have been formed in every health evangelism program I have conducted. From these friendships new church members are acquired.
Traditional evangelistic efforts are usually conducted by a charismatic preacher who carries the burden of presenting truth, pretty much by himself. Usually, there are no small groups and no meaningful interface between church members and the public who come to these large meetings. This method of evangelism fails to create friendships between church members and the public who attend these meetings.
In traditional evangelistic efforts, if local church members are involved, they are usually relegated to the role of helping to swell the audience, pray for the meetings, or perhaps usher and take up an offering. There is no specific activity in traditional evangelistic meetings designed for individuals from the public to create friendships with church members. This is one of the reasons why so many new members leave the church shortly after the meetings are past. They simply do not have any friends in the church they have just joined. The evangelist is gone to another city. The new church member just got baptized into a church of total strangers.
Newly baptized church members are more likely to stay if they have at least one good friend in the church. Health evangelism programs featuring small group interactions between the public and church members creates one-on-one relationships and sustains them. Solid, lasting friendships are formed. Baptisms resulting from health evangelism programs where friendships are made are much more likely to stay in the church than baptisms resulting from traditional evangelistic activities.
Health evangelism programs will prepare community people to be exposed to more traditional evangelistic meetings at some subsequent time. Health evangelism and traditional evangelistic meetings should not be piggy backed one on the other, but each should be conducted often enough that those who are ready for indoctrination can avail themselves of a traditional evangelistic crusade.
What I have found works best is for health evangelism programs to be offered on a regular, continuing basis on one track and traditional evangelistic efforts at regular intervals on another track. The purpose of each track is clear. The health evangelism track is health oriented, but creates firm friendships with church members and introduces a person to God as the agent of behavior change in the daily life. The traditional evangelistic crusade track is for the purpose of broadening the spiritual understanding and experience of an individual along doctrinal lines. This prepares a person for full membership in the church.
Soul-saving friendships can be built in small groups that meet each session of a health evangelism program. Lasting friendships with men and women from the community have been formed in every health evangelism program I have conducted. From these friendships new church members are acquired.
Traditional evangelistic efforts are usually conducted by a charismatic preacher who carries the burden of presenting truth, pretty much by himself. Usually, there are no small groups and no meaningful interface between church members and the public who come to these large meetings. This method of evangelism fails to create friendships between church members and the public who attend these meetings.
In traditional evangelistic efforts, if local church members are involved, they are usually relegated to the role of helping to swell the audience, pray for the meetings, or perhaps usher and take up an offering. There is no specific activity in traditional evangelistic meetings designed for individuals from the public to create friendships with church members. This is one of the reasons why so many new members leave the church shortly after the meetings are past. They simply do not have any friends in the church they have just joined. The evangelist is gone to another city. The new church member just got baptized into a church of total strangers.
Newly baptized church members are more likely to stay if they have at least one good friend in the church. Health evangelism programs featuring small group interactions between the public and church members creates one-on-one relationships and sustains them. Solid, lasting friendships are formed. Baptisms resulting from health evangelism programs where friendships are made are much more likely to stay in the church than baptisms resulting from traditional evangelistic activities.
Health evangelism programs will prepare community people to be exposed to more traditional evangelistic meetings at some subsequent time. Health evangelism and traditional evangelistic meetings should not be piggy backed one on the other, but each should be conducted often enough that those who are ready for indoctrination can avail themselves of a traditional evangelistic crusade.
What I have found works best is for health evangelism programs to be offered on a regular, continuing basis on one track and traditional evangelistic efforts at regular intervals on another track. The purpose of each track is clear. The health evangelism track is health oriented, but creates firm friendships with church members and introduces a person to God as the agent of behavior change in the daily life. The traditional evangelistic crusade track is for the purpose of broadening the spiritual understanding and experience of an individual along doctrinal lines. This prepares a person for full membership in the church.
Baptism: Event or Process?
Baptisms are events that can be easily measured and are carefully counted. The effectiveness of a pastor’s ministry is often equated with the number of baptisms that are produced by their ministry. But counting baptisms alone is a bit near sighted because it ignores the long process that leads up to baptism and also ignores the process of discipling that should follow.
Becoming a Christian is not just an isolated event but a process. Baptism is a single point along a continuum. We put too much emphasis on baptism and tend to ignore the processes that come before and after. There are many measurable points in the process leading to baptism. Health evangelism programs lead people through many of these initial steps.
Those who conduct health evangelism programs should measure these intermediate steps that lead to baptism. When this is done, the value of health evangelism will be demonstrated. What are some of these intermediate steps?
What does your church do? Sabbath services are probably the most notable thing your church does. Frankly, services in your church will not be of much interest to anyone who goes to their own church on a regular basis.
Health evangelism will make your church more attractive because few churches do anything for the health of the community. If your church regularly helped people stop smoking, lose weight, reverse diabetes or hypertension or other chronic lifestyle related disease, that would make your church more attractive to those struggling with these problems.
The more health evangelism activities you conduct, the more interest the community will have in your church. This would simply be a social gospel if your help was solely physical or mental in nature. Each of your community activities should point to Jesus as the agent of lasting behavior change in the human life. When you do this, then you are conducting true health evangelism.
The very first step in a person becoming a member of your church is developing an interest in something you do in your church. So, start doing something. Do it often, do it well, and do it regularly. The community will flock to your church.
This is another obvious step in becoming a church member. Health evangelism programs help people take this step if your health evangelism program is conducted in the local church.
When a person comes to a health evangelism program in your church they must get directions, drive to your church, find a parking spot, find the right entrance, come through the door, and say “hello” to someone. It is much less threatening for a person in the community to come to your church for a health evangelism program on a week night than to come to regular religious services on the weekend.
If you provide specific help for a specific health problem at your church, the community will come. At some time in the future, when they have made friends with church members, they will find it much easier to come to your church for religious services because they know how to get to your church, where to park, which door to come through, they will recognize people and will even know where the restrooms are located.
This step toward baptism is as easy to measure as baptisms. Keeping statistics on the number of non-church member visits to your church will be a measure of the effectiveness of your health evangelism program. These numbers will help pastors and church administrators see the value of health evangelism programs.
Count every visit by every non-church member every time they step through your door. If 20 non-church members attend a 5-Day Plan to Stop smoking for 5 nights that equals 100 non-church member visits to your church. This can simply be called the “non-Adventist person visit” or NAPV.
Most health education programs provide accurate health and medical information, but have been poor at providing personal contact with church members. I believe that health evangelism programs should be designed to maximize the interface between church members and the public. This is the one factor that will change them from being primarily informational to being interactive and evangelistic.
Each church member (health ministry volunteer) who helps with your health evangelism program should be assigned to 3-4 community participants. Sufficient time should be created in the health evangelism program for church members to interact with the individuals from the community. Give church members real but simple work to do. Let them review the high points of the night’s lecture. Let them ask individuals what they personally have decided to do in their own lives as a result of the lecture.
Give the church members time to get some feedback from the participants in small groups. Let them listen to their struggles and hardships. Teach them to have a sympathetic ear. Teach them to be nonjudgmental. Teach them to be friends. This is not hard for church members to learn or to do. This type of friendship activity is not at all like giving formal Bible studies. Give church members a list of questions to ask and teach them to listen and be sympathetic. This is how friendships are formed.
This is a step toward baptism that can be measured. Count each church member contact with a non-church member as a friendship interaction. This is another step toward baptism that results from health evangelism programs. Contact could be by phone, text, email, or in person. Each interaction of this type should be counted and entered into your program’s database.
This is probably the most important step in any health evangelism program. If you become a church member without taking this step, you are a Christian only in name. Church membership is equated with developing a personal relationship with God. Where and when does this relationship with God occur? Baptism is the public step that indicates that an individual has made a full commitment to Jesus, but baptism doesn’t make it happen.
Health evangelism programs are an ideal setting in which a person can get to know Jesus. People come to health evangelism programs because they have a behavioral problem that needs to be changed. The program provides information your audience needs to know to make changes in how they live. You provide individual counseling and friendship through your church members, but the audience needs more.
In every health evangelism program there should be simple, specific information on how Jesus helps people change behavior. This evangelistic approach should be very specific and narrowly focused on the behavioral problem the participant is trying to overcome. Many will find that Jesus is an ever present help in time of need in a health evangelism program, but only if you design it that way.
Information about Jesus, with an opportunity to apply His help to a specific problem, puts problem-specific evangelism into health education and creates a health evangelism program. If people find that God helps them in tangible ways in a health evangelism program, they will be much more inclined to join your church once they have been introduced to the distinctive doctrines.
This step toward baptism can be measured but is a bit more difficult. In your questionnaire following the health evangelism program, and in each of the follow-up visits you can ask people what their relationship with Jesus is with respect to the problem they were trying to overcome. Many will confess that they have a new or deeper relationship with Jesus as a result of your health evangelism program. They will share that they never would have been successful in changing their behavior unless they had received God’s help.
This is one more step in the process leading to baptism. We shouldn’t baptize anyone who doesn’t have an experiential relationship with Jesus. Too often we baptize people who intellectually give assent to a body of doctrines but who have no real experience of God’s power in their lives.
Obviously, health evangelism programs are about changing the way you live. Many health destroying habits and addictions can be changed in a health evangelism program. A healthier lifestyle free from addictions is another step toward baptism, and it is quite easy to measure.
This is the last step in the process before baptism. To be a church member in regular standing, it is necessary to accept the distinctive doctrines of the church. Learning the distinctive doctrines is not a function of health evangelism except for the doctrines dealing with healthful living.
At last, a person joins the church by baptism. We all rejoice! This is the main goal of the church. The church is to proclaim the gospel of Jesus Christ and to baptize those who believe on His name.
Is it fair to ask those who conduct health evangelism programs, “Where are the baptisms?” Not really. The question reveals an ignorance of the processes that lead to baptism. Such a question reveals a lack of appreciation for the ways in which health evangelism prepares people for baptism.
Of the seven steps leading to baptism I have outlined above, health evangelism leads people through the first five. That should be good enough. Health evangelism is only the right hand of the gospel not the whole gospel. Health evangelism opens doors, makes friends, and gives people an experiential relationship with Jesus but it does not fully indoctrinate them or directly result in baptisms.
Health evangelism can be understood as being “problem specific” evangelism. You can be “saved” spiritually in a health evangelism program, but it is “getting saved” over just one behavioral problem, not all of life’s problems. We all started our journey toward God at some point. Health evangelism can be the starting point for many. A rudimentary experience with God, developed in overcoming a specific health problem, can over time and spiritual growth lead to a fuller experience.
Your church should hold health evangelism programs that are designed and conducted in the way that will guide people along the steps leading to baptism. Do not say that health evangelism programs are not evangelistic. Health evangelism is focused evangelism that helps people (turn to God for dealing) with specific addictions and habits.
I had one lady who came from a secular background, but experimenting with prayer she successfully quit smoking with God’s help. In asking her about her success she said, “This is a model of behavior change that I can now apply to other problem areas in my life.” That would be the process of “sanctification” in more traditional theological terms. She had learned that God had helped her with one problem and she was now ready to expand her experience with God and overcome in other areas as well.
Exactly when and how a person comes to God is a mystery to us who do His work. We are wise if we realize there are many ways people can initiate a relationship with God. We need to recognize that every human necessity is an opportunity to introduce a person to God who helps with every need.
Becoming a Christian is not just an isolated event but a process. Baptism is a single point along a continuum. We put too much emphasis on baptism and tend to ignore the processes that come before and after. There are many measurable points in the process leading to baptism. Health evangelism programs lead people through many of these initial steps.
Those who conduct health evangelism programs should measure these intermediate steps that lead to baptism. When this is done, the value of health evangelism will be demonstrated. What are some of these intermediate steps?
- Step 1. An interest in something you do in your church.
What does your church do? Sabbath services are probably the most notable thing your church does. Frankly, services in your church will not be of much interest to anyone who goes to their own church on a regular basis.
Health evangelism will make your church more attractive because few churches do anything for the health of the community. If your church regularly helped people stop smoking, lose weight, reverse diabetes or hypertension or other chronic lifestyle related disease, that would make your church more attractive to those struggling with these problems.
The more health evangelism activities you conduct, the more interest the community will have in your church. This would simply be a social gospel if your help was solely physical or mental in nature. Each of your community activities should point to Jesus as the agent of lasting behavior change in the human life. When you do this, then you are conducting true health evangelism.
The very first step in a person becoming a member of your church is developing an interest in something you do in your church. So, start doing something. Do it often, do it well, and do it regularly. The community will flock to your church.
- Step 2. Come to your church.
This is another obvious step in becoming a church member. Health evangelism programs help people take this step if your health evangelism program is conducted in the local church.
When a person comes to a health evangelism program in your church they must get directions, drive to your church, find a parking spot, find the right entrance, come through the door, and say “hello” to someone. It is much less threatening for a person in the community to come to your church for a health evangelism program on a week night than to come to regular religious services on the weekend.
If you provide specific help for a specific health problem at your church, the community will come. At some time in the future, when they have made friends with church members, they will find it much easier to come to your church for religious services because they know how to get to your church, where to park, which door to come through, they will recognize people and will even know where the restrooms are located.
This step toward baptism is as easy to measure as baptisms. Keeping statistics on the number of non-church member visits to your church will be a measure of the effectiveness of your health evangelism program. These numbers will help pastors and church administrators see the value of health evangelism programs.
Count every visit by every non-church member every time they step through your door. If 20 non-church members attend a 5-Day Plan to Stop smoking for 5 nights that equals 100 non-church member visits to your church. This can simply be called the “non-Adventist person visit” or NAPV.
- Step 3. Become friends with church members.
Most health education programs provide accurate health and medical information, but have been poor at providing personal contact with church members. I believe that health evangelism programs should be designed to maximize the interface between church members and the public. This is the one factor that will change them from being primarily informational to being interactive and evangelistic.
Each church member (health ministry volunteer) who helps with your health evangelism program should be assigned to 3-4 community participants. Sufficient time should be created in the health evangelism program for church members to interact with the individuals from the community. Give church members real but simple work to do. Let them review the high points of the night’s lecture. Let them ask individuals what they personally have decided to do in their own lives as a result of the lecture.
Give the church members time to get some feedback from the participants in small groups. Let them listen to their struggles and hardships. Teach them to have a sympathetic ear. Teach them to be nonjudgmental. Teach them to be friends. This is not hard for church members to learn or to do. This type of friendship activity is not at all like giving formal Bible studies. Give church members a list of questions to ask and teach them to listen and be sympathetic. This is how friendships are formed.
This is a step toward baptism that can be measured. Count each church member contact with a non-church member as a friendship interaction. This is another step toward baptism that results from health evangelism programs. Contact could be by phone, text, email, or in person. Each interaction of this type should be counted and entered into your program’s database.
- Step 4. Develop or strengthen a relationship with God.
This is probably the most important step in any health evangelism program. If you become a church member without taking this step, you are a Christian only in name. Church membership is equated with developing a personal relationship with God. Where and when does this relationship with God occur? Baptism is the public step that indicates that an individual has made a full commitment to Jesus, but baptism doesn’t make it happen.
Health evangelism programs are an ideal setting in which a person can get to know Jesus. People come to health evangelism programs because they have a behavioral problem that needs to be changed. The program provides information your audience needs to know to make changes in how they live. You provide individual counseling and friendship through your church members, but the audience needs more.
In every health evangelism program there should be simple, specific information on how Jesus helps people change behavior. This evangelistic approach should be very specific and narrowly focused on the behavioral problem the participant is trying to overcome. Many will find that Jesus is an ever present help in time of need in a health evangelism program, but only if you design it that way.
Information about Jesus, with an opportunity to apply His help to a specific problem, puts problem-specific evangelism into health education and creates a health evangelism program. If people find that God helps them in tangible ways in a health evangelism program, they will be much more inclined to join your church once they have been introduced to the distinctive doctrines.
This step toward baptism can be measured but is a bit more difficult. In your questionnaire following the health evangelism program, and in each of the follow-up visits you can ask people what their relationship with Jesus is with respect to the problem they were trying to overcome. Many will confess that they have a new or deeper relationship with Jesus as a result of your health evangelism program. They will share that they never would have been successful in changing their behavior unless they had received God’s help.
This is one more step in the process leading to baptism. We shouldn’t baptize anyone who doesn’t have an experiential relationship with Jesus. Too often we baptize people who intellectually give assent to a body of doctrines but who have no real experience of God’s power in their lives.
- Step 5. Change certain behaviors.
Obviously, health evangelism programs are about changing the way you live. Many health destroying habits and addictions can be changed in a health evangelism program. A healthier lifestyle free from addictions is another step toward baptism, and it is quite easy to measure.
- Step 6. Accept Distinctive Doctrines.
This is the last step in the process before baptism. To be a church member in regular standing, it is necessary to accept the distinctive doctrines of the church. Learning the distinctive doctrines is not a function of health evangelism except for the doctrines dealing with healthful living.
- Step 7. Baptism.
At last, a person joins the church by baptism. We all rejoice! This is the main goal of the church. The church is to proclaim the gospel of Jesus Christ and to baptize those who believe on His name.
Is it fair to ask those who conduct health evangelism programs, “Where are the baptisms?” Not really. The question reveals an ignorance of the processes that lead to baptism. Such a question reveals a lack of appreciation for the ways in which health evangelism prepares people for baptism.
Of the seven steps leading to baptism I have outlined above, health evangelism leads people through the first five. That should be good enough. Health evangelism is only the right hand of the gospel not the whole gospel. Health evangelism opens doors, makes friends, and gives people an experiential relationship with Jesus but it does not fully indoctrinate them or directly result in baptisms.
Health evangelism can be understood as being “problem specific” evangelism. You can be “saved” spiritually in a health evangelism program, but it is “getting saved” over just one behavioral problem, not all of life’s problems. We all started our journey toward God at some point. Health evangelism can be the starting point for many. A rudimentary experience with God, developed in overcoming a specific health problem, can over time and spiritual growth lead to a fuller experience.
Your church should hold health evangelism programs that are designed and conducted in the way that will guide people along the steps leading to baptism. Do not say that health evangelism programs are not evangelistic. Health evangelism is focused evangelism that helps people (turn to God for dealing) with specific addictions and habits.
I had one lady who came from a secular background, but experimenting with prayer she successfully quit smoking with God’s help. In asking her about her success she said, “This is a model of behavior change that I can now apply to other problem areas in my life.” That would be the process of “sanctification” in more traditional theological terms. She had learned that God had helped her with one problem and she was now ready to expand her experience with God and overcome in other areas as well.
Exactly when and how a person comes to God is a mystery to us who do His work. We are wise if we realize there are many ways people can initiate a relationship with God. We need to recognize that every human necessity is an opportunity to introduce a person to God who helps with every need.